Oral Hygiene
Babies do not produce very much saliva during the first two months of life.
With a cleft palate, milk can enter the nose during feeds, and while breast milk does not irritate the delicate tissue here, formula milk can leave deposits which may result in a snuffly baby. Formula-fed babies may require 2/3 teaspoons of cooled boiled water after a feed to ensure that any milk is removed from the nasal airways.
Children with a cleft which affects their gums are especially vulnerable to tooth decay, as the position of their teeth can be crooked or twisted at and therefore harder to clean. As they grow older and get their milk teeth, maintaining good oral hygiene by cutting down on sugar and regularly visiting the dentist is essential.
Cleft lip
Babies born with a cleft lip alone usually feed well. Some babies breastfeed better with the cleft facing upwards. The breast tissue usually fills the gap where the cleft is and allows efficient feeding. Some bottle fed babies feed better on a wide based teat. If cleft is unilateral, use of modified football method or straddle position (Fig. 1) may be helpful.

Fig. 1 straddle position *
Cleft palate
The palate, more commonly referred to as the roof of the mouth, separates the mouth from the nose. The palate is important for feeding and speaking. A cleft is an opening or split in the palate. This cleft can make feeding hard for your baby. Most babies with a cleft of the palate are not able to use standard bottles or solely breast feed because they cannot create the suction needed to draw the milk out of the nipple. Special bottles and nipples are available to help infants with cleft palate feed and grow. These bottles may be used with formula or breast milk.
Breastfeeding
Learning that breastfeeding is an unlikely option can be a source of disappointment and sadness for some families. Give yourself time and space to grieve this loss. But remember, you can still share many benefits of breastfeeding with your child:
• Express breast milk with a pump, but feed your baby with one of the bottle-feeding methods described.
• During feedings, make sure that you both enjoy eye-to-eye, and skin-to-skin contact whenever possible.
• Once your baby has become successful feeding on a bottle, she may be put to the breast for non-nutritive sucking. Non-nutritive sucking at the breast can be a satisfying experience for both moms and babies.
• Non-nutritive sucking exercises and stimulates important muscles in your baby’s mouth and tongue, and can facilitate the bonding experience. It may also help stimulate milk production for those moms who continue to pump breast milk.
‘Dancer hand position’ is recommended (Fig. 2). Slide the hand under the breast forward, i.e. supporting the breast with three fingers rather than four form a U-shape with the thumb and forefinger to cradle the baby's chin, this helps the baby to press the nipple and areola between the gums.
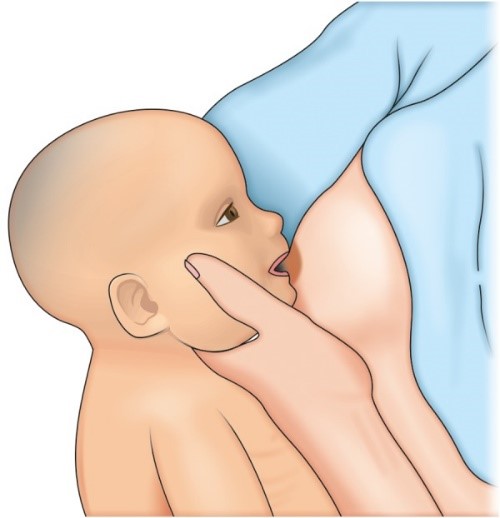
Fig. 2 Dancer hand position*
Bottle Manufacturers
Consult with the Cleft Clinic to choose the right bottle for your baby. Based on your baby's cleft type and feeding skills, one of following bottles may be recommended:
-Dr. Brown’s Specialty Feeding System® (https://www.drbrownsbaby.com/medical/products/specialty-feeding/)
-Mead Johnson Cleft Palate Nurser (http://shop.enfamil.com/accessories/)
-Medela SpecialNeeds® Feeder (https://www.medelabreastfeedingus.com/products/576/specialneeds-feeder)
-Haberman Feeder (https://www.youtube.com/watch?v=QgqKAgRiNDY)
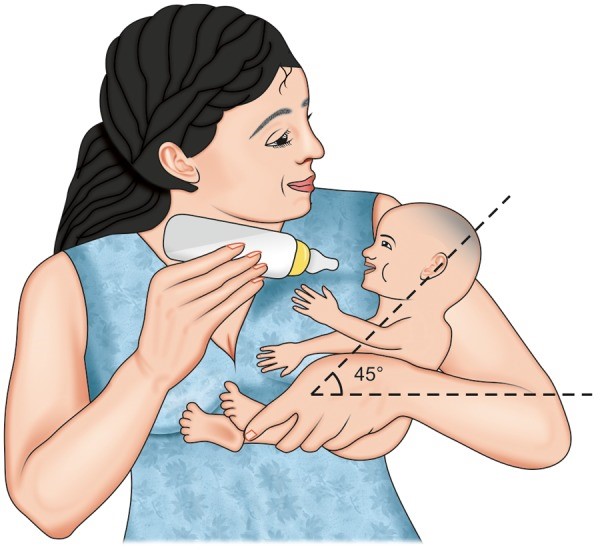
Fig. 3 Correct position of feeding*
How much should my baby eat?
Newborn babies begin with frequent feedings of very small amounts of milk (1 ounce or less). Over time, they increase the amount they can take.
By 2 weeks of age, a baby needs at least 2 to 2.5 ounces of milk per pound of weight each day. For example, a 3-week old baby who weighs 9 pounds should have at least 18 to 22.5 ounces of breast milk or formula in 24 hours.
A feeding session should take no longer than 30 minutes. If it takes longer, your baby is working too hard and burning calories needed for growth.
We recommend weighing babies weekly until they show a normal rate of growth. Usually this happens in 4 to 6 weeks.
How often does my baby need to eat?
During the first month of life, a baby will feed 8 to 12 times per day — every 2 to 3 hours. A baby this young usually feeds at least 2 times during the night.
At 2 to 4 months, a baby will feed 6 to 8 times per day — every 3 to 4 hours.
How will I know if my baby is gaining enough weight?
A baby usually loses weight the first week of life. The loss is usually 5% to 10% of their body weight. Your baby should regain this weight by 2 weeks old.
At first, we expect your baby to gain 5 to 7 ounces per week. At 4 to 6 months old, the rate of weight gain slows. Your baby should gain about 3.5 to 4.5 ounces per week.
What about starting solid foods?
Babies with clefts can start solid foods at the same age as other babies. Most often, this is at 4 to 6 months.
Experiment to find the right consistency for solids. It needs to be just right so your baby can eat without the food coming out their nose. This is not harmful to your baby. Sneezing will usually clear the food out of the nose. Most babies learn quickly to get the food down their throats rather than out their noses.
Can my baby drink from a cup?
Cup feeding can also be started at the usual age, 8 to 12 months. Cups with plain lids can help limit spills. Do not use spill-proof cups with valves. These require that baby create suction to get any fluid.
Feeding Your Baby Videos
https://cleftline.org/family-resources/feeding-your-baby/feeding-your-baby-videos/
PROSTHESIS
Feeding obturators are passive devices designed to provide a normal contour to the patients of cleft alveolus and hard palate. They separate the oral and nasal cavities and provide a surface to oppose the nipple. Obturators have been a major area of controversy. There are two schools of thoughts, the first one advocates its advantages – that they help in feeding, facilitate lip and palate repair, speech and facial growth are enhanced. The other group claims its disadvantages–its impression taking procedure too cumbersome for the infant, second most important criteria is its sterilization and hygiene maintenance. To date there is no evidence to support or disown its use. The practice remains empirical.
Summarize:
When to Call the SLP
Call our feeding team or your child's doctor if your baby has:
*Jindal, M. K., & Khan, S. Y. (2013). How to feed cleft patient?. International Journal of Clinical Pediatric Dentistry, 6(2), 100.
